Breakthrough
Procedure
Home
Procedures
Procedures
⋅
Non-Traumatic Procedures: Lumbar
⋅
Non-Traumatic Procedures: Cervical
⋅
Other Procedures: Lumbar
⋅
Other Procedures: Cervical
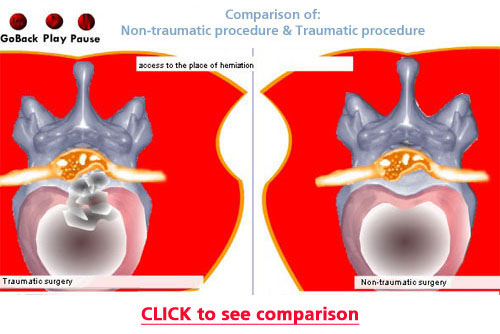
Difference between LUMBAR Non-traumatic procedure and Traumatic procedure
Conditions
Conditions
⋅
Back Pain
⋅
Bone Spurs
⋅
Bulging Disc
⋅
Degenerative Disc Disease
⋅
Failed Back Surgery Syndrome
⋅
Herniated Disc
⋅
Neck Pain
⋅
Pinched Nerve
⋅
Prolapsed Disc
⋅
Radiculopathy
⋅
Slipped Disc
⋅
Sciatica
⋅
Spinal Stenosis
⋅
Spondylolisthesis
About BI
About Back Institute
⋅
Why Choose Back Institute
⋅
New Surgical Technique
⋅
Publications - Peer Reviewed
⋅
Patient Testimonials
⋅
Library: Book Chapter, Video, Pictures, Articles
⋅
Back Institute Founder
⋅
Mission Statement
⋅
Contact BI
72 Hours
Resources
Resources
⋅
Am I a Candidate
⋅
Frequently Asked Questions
⋅
Questions to Ask Your Doctor
⋅
Free MRI / CT Scan Review
⋅
Library: Book Chapter, Video, Pictures, Articles
⋅
Hype Debunked
⋅
Where Do Medical Doctors Have Surgery
⋅
What Some Other Centers Do
Comparison Table (outpatient spine surgery centers)
Avoid Hype
Caution
(1) LASER
(2) TRAUMATIC SPINE SURGERY
Testimonials
Testimonials
- NON-TRAUMATIC SPINE PROCEDURE TESTIMONIALS
Listen to real patients talk about their experiences at Back Institute.
Forms
(1)
New Patient Form
- Let us Help to Solve Your Problem
This is a CONFIDENTIAL questionnaire to help us determine
the best treatment plan for you. Please fill out this questionnaire
as completely as possible.
(2)
Incoming Patient Form
: This area is only for the patients
who set surgery date with us.
(3)
Existing Patient Forms
- Post Surgery Forms
This area is only for the patients
who had surgery with us
.
This will help you to follow the best rehabilitative protocol.
Contact
Evaluation, education or treatment locations:
Toll Free : 800.956.6724
Email :help@backinstitute.com
More than 1 Week Post surgery form
This area is only for the patients who had surgery with us.
Contact Information:
Name
Email
Age
Occupation
City
State
Medical Information:
Today's Date(mm/dd/yy)
Date of surgery(mm/dd/yy)
Do you have occasional back or leg pain (neck or arm pain, if it was a neck problem) severe enough to interfere with normal work or leisure activities?
Yes
No
Are you handicapped by severe pain?
Yes
No
How are your symptoms different
in comparison to prior to your procedure?
What medication are you taking and how often?
Are you having or have you had any physical therapy(at home or at a therapy center?)Please describe:
When did you return to work?
Are you working at the same job as prior to the start of your back problem? If a different job, please describe:
Working full time?
No limitation or if there is a limitation at work, please describe:
© 1995 - 2014 BackInstitute.com
Any questions about this site, mail to
Webmaster.
|
Privacy Policy